The COVID-19 pandemic calls out for international cooperation. Countries aren’t listening.
By Jadenne Radoc Cabahug
Lack of international cooperation has slowed recovery in "developing" countries still wrestling with mutating strains of COVID-19, slowing full global recovery and extending real human suffering.
“It's very important for all of us to know the big toll of COVID-19 [to] help with planning,” Dr. Ali Mokdad, professor of Global Health at the Institute for Health Metrics (IHME) at the University of Washington said. “Rich countries need to help poor countries and make sure that resources are allocated appropriately.”
The COVID-19 pandemic reached every nook and cranny of the world in the span of a few months.
Despite its far global reach and impact on every person in the world, countries did not cooperate at the emergence and height of the pandemic. While some countries have been lucky enough to begin stemming the worst effects of the disease, others are still struggling to lower case numbers and fight new stronger waves of infection.
From the beginning, countries were ill prepared to handle the fast-spreading disease. The 2019 Johns Hopkins Global Health Security Index found that no country was fully prepared for a coronavirus outbreak. The United States received top scores as one of the countries most prepared for a pandemic, however, it is the country with the most COVID-19 cases in the world. Many administrations were slow to react, to close borders for travel and prepare healthcare systems to adequately meet the challenge.
Even in countries like the United States, healthcare systems were overwhelmed with COVID-19 cases. They lacked ready supplies of personal protective equipment and infection test kits, tracing procedures and vaccines.
Ruanne Barnabas, associate professor in the Department of Global Health and Division of Allergy and Infectious Diseases at the University of Washington, says that public health inequities between developed and developing nations are stark.
“It's very important for all of us to know the big toll of COVID-19 [to] help with planning,” Dr. Ali Mokdad, professor of Global Health at the Institute for Health Metrics (IHME) at the University of Washington said. “Rich countries need to help poor countries and make sure that resources are allocated appropriately.”
The COVID-19 pandemic reached every nook and cranny of the world in the span of a few months.
Despite its far global reach and impact on every person in the world, countries did not cooperate at the emergence and height of the pandemic. While some countries have been lucky enough to begin stemming the worst effects of the disease, others are still struggling to lower case numbers and fight new stronger waves of infection.
From the beginning, countries were ill prepared to handle the fast-spreading disease. The 2019 Johns Hopkins Global Health Security Index found that no country was fully prepared for a coronavirus outbreak. The United States received top scores as one of the countries most prepared for a pandemic, however, it is the country with the most COVID-19 cases in the world. Many administrations were slow to react, to close borders for travel and prepare healthcare systems to adequately meet the challenge.
Even in countries like the United States, healthcare systems were overwhelmed with COVID-19 cases. They lacked ready supplies of personal protective equipment and infection test kits, tracing procedures and vaccines.
Ruanne Barnabas, associate professor in the Department of Global Health and Division of Allergy and Infectious Diseases at the University of Washington, says that public health inequities between developed and developing nations are stark.

COVID Center in Saint Malo. Via Eloïse Pouleau.
Tracking trends
Global COVID-19 trends are difficult to follow due to a lack of testing. Most countries with high population densities report low COVID-19 case numbers because residents lack easy access to hospitals and/or COVID testing.
In the case of India, which has a high population density and high COVID-19 cases, “It really is this kind of perfect storm of having a transmissible enough virus, enough mobility, enough contact,” Barnabas said. “Without the rapid response to increasing numbers of cases that allow these events like in India, these very big political meetings and rallies or other types of big events where people are congregating, those really put people at risk and, and have resulted in, in large numbers of cases.”
The countries with the highest COVID-19 cases are the United States, India, Brazil, France, and Turkey, according to Worldometer.
A study conducted by the UW IHME is the first of its kind to attempt to estimate the true global death toll of COVID-19. It found that actual COVID-19 death numbers could range from double to ten times as much as the reported numbers.
The United States, India, Mexico, Brazil, and Russia are the countries with the highest estimated death tolls. These estimated numbers are double, or ten times the currently reported numbers.
The IHME used data from 59 countries to show that 6.9 million people have died from COVID-19, double the number reported by the World Health Organization.
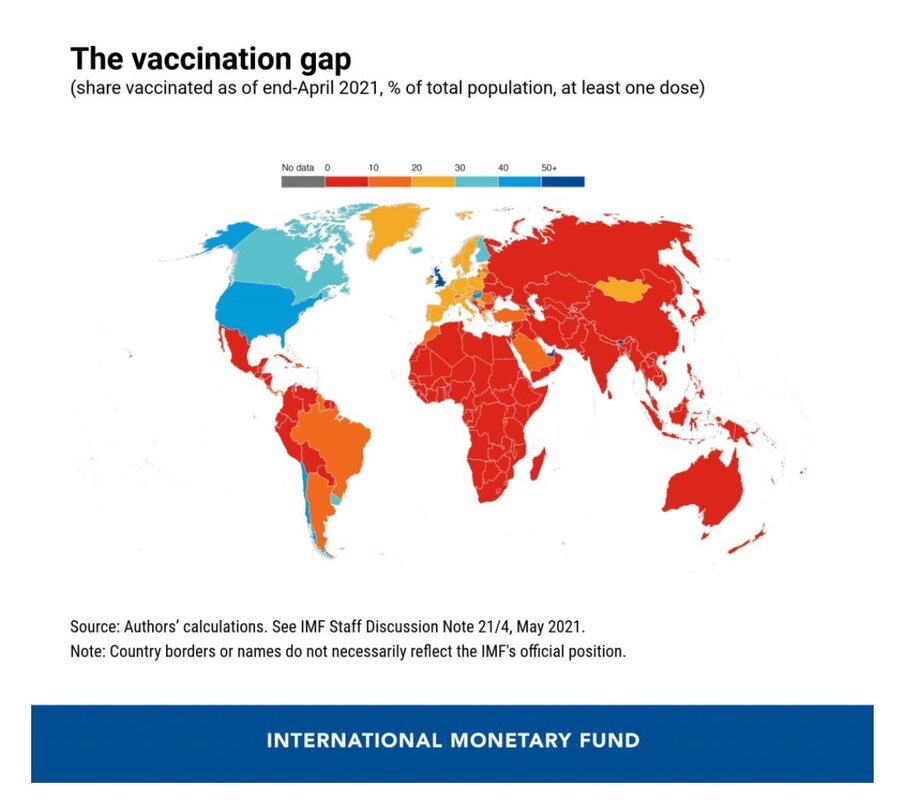
As developed nations buy and distribute vaccines widely throughout their countries as well as push for the possibility of booster vaccines, developing nations are seeing a surge of COVID-19 cases, deaths, and mutated variants.
The United States seems to be well on its way to vaccinating 70 percent of its population by President Biden’s July 4 deadline, but other parts of the world are still in the early stages of vaccination program rollouts.
A pandemic, by definition, calls out for international cooperation. Instead, countries responded with a patchwork approach that delivered uneven results and successive waves of illness and death.
Global COVID-19 trends are difficult to follow due to a lack of testing. Most countries with high population densities report low COVID-19 case numbers because residents lack easy access to hospitals and/or COVID testing.
In the case of India, which has a high population density and high COVID-19 cases, “It really is this kind of perfect storm of having a transmissible enough virus, enough mobility, enough contact,” Barnabas said. “Without the rapid response to increasing numbers of cases that allow these events like in India, these very big political meetings and rallies or other types of big events where people are congregating, those really put people at risk and, and have resulted in, in large numbers of cases.”
The countries with the highest COVID-19 cases are the United States, India, Brazil, France, and Turkey, according to Worldometer.
A study conducted by the UW IHME is the first of its kind to attempt to estimate the true global death toll of COVID-19. It found that actual COVID-19 death numbers could range from double to ten times as much as the reported numbers.
The United States, India, Mexico, Brazil, and Russia are the countries with the highest estimated death tolls. These estimated numbers are double, or ten times the currently reported numbers.
The IHME used data from 59 countries to show that 6.9 million people have died from COVID-19, double the number reported by the World Health Organization.
As developed nations buy and distribute vaccines widely throughout their countries as well as push for the possibility of booster vaccines, developing nations are seeing a surge of COVID-19 cases, deaths, and mutated variants.
The United States seems to be well on its way to vaccinating 70 percent of its population by President Biden’s July 4 deadline, but other parts of the world are still in the early stages of vaccination program rollouts.
A pandemic, by definition, calls out for international cooperation. Instead, countries responded with a patchwork approach that delivered uneven results and successive waves of illness and death.

Effectiveness factors
Development status of a country is not the sole determinant of how well a state handles the virus. The way countries handled case numbers depended on government and public health administrations.
In the United States, President Biden has received higher marks from Americans for his handling of the pandemic than did former President Trump, according to a study by Northeastern, Harvard, Northwestern, and Rutgers.
In many countries, the pandemic became politicized, causing a division between party affiliations.
In New Zealand, the strategy of community and cooperation was used to stop the spread of the virus.
Kushil McPherson is a law school student at the University of Auckland, New Zealand. She said during the pandemic, New Zealand used the Māori saying, “kia kaha,” which means stay strong.
“We really incorporated all of the central ideas of Māori culture and language into our actions as a country to try to keep each other safe,” McPherson said. “Everyone just did it really well and I'm really proud of how everyone handled things here.”
McPherson said that New Zealanders worked with the government at every step of the way to prevent community cases. The current state of New Zealand looks like a pre-COVID world. People are free to roam sans masks, social distancing, and COVID testing.
The New Zealand government was strict on mass testing and tracing through apps like the NZ COVID Tracer App. People would scan barcode signs on their phones using the app to track the exact time and location if there is a case.
New Zealand is considered a developed nation with the advantage of being surrounded by water.
Barnabas said the New Zealand government was very strict on restrictions and is highly responsive to any cases that emerge.
Development status of a country is not the sole determinant of how well a state handles the virus. The way countries handled case numbers depended on government and public health administrations.
In the United States, President Biden has received higher marks from Americans for his handling of the pandemic than did former President Trump, according to a study by Northeastern, Harvard, Northwestern, and Rutgers.
In many countries, the pandemic became politicized, causing a division between party affiliations.
In New Zealand, the strategy of community and cooperation was used to stop the spread of the virus.
Kushil McPherson is a law school student at the University of Auckland, New Zealand. She said during the pandemic, New Zealand used the Māori saying, “kia kaha,” which means stay strong.
“We really incorporated all of the central ideas of Māori culture and language into our actions as a country to try to keep each other safe,” McPherson said. “Everyone just did it really well and I'm really proud of how everyone handled things here.”
McPherson said that New Zealanders worked with the government at every step of the way to prevent community cases. The current state of New Zealand looks like a pre-COVID world. People are free to roam sans masks, social distancing, and COVID testing.
The New Zealand government was strict on mass testing and tracing through apps like the NZ COVID Tracer App. People would scan barcode signs on their phones using the app to track the exact time and location if there is a case.
New Zealand is considered a developed nation with the advantage of being surrounded by water.
Barnabas said the New Zealand government was very strict on restrictions and is highly responsive to any cases that emerge.

Janine Radoc and her family celebrating Christmas online. Via Janine Radoc
Corruption and tears
“We copied what was done by other countries related to restrictions and regulations,” said Tankiso Motipi, a Civil Registration Officer at the Ministry of Home Affairs in Maseru, Lesotho. “But when it comes to the government going on out to prepare for all the resources, we provided zero resources.”
She said the government of Lesotho was quick to react and follow pandemic procedures, but it failed at the administrative and public health level. Motipi said the first case appeared around October 2020, so the government had time to prepare for cases, unlike other parts of the world.
“There was nothing that we did to prepare for such an event, and all we could do was just cry,” Motipi said.
The government promised to provide masks, hand sanitizer, test kits, and other essential PPE items to reduce the spread of the virus through a government fund and donations, but Motipi said citizens never received any of it.
With little information given to inform the public about the virus, most people were uncertain of everything. The news of the virus didn’t reach the most rural parts of Lesotho until much later in the pandemic.
“At first, it was panic. We were all panicking, we were paranoid. I mean, the whole country because we didn't even know what we were dealing with.”
Motipi said most Lesotho citizens do not have medical aid or insurance. Only people who can afford it have medical insurance.
When it comes to testing for the virus, most people can’t afford to test if they display symptoms because it’s done privately.
Motipi described the only two ways to test publicly, which would be if an elderly person is traveling to receive pension or if someone with severe symptoms of the virus was referred to South Africa for treatment. Those are the only ways to test in a public hospital for free.
“We have only one ICU unit in the country in the biggest hospital which, by the way, is a referral hospital,” Motipi said. “You don't just run to that hospital and say hello, I'm sick. Someone has to refer you and the ICU unit has only nine beds.”
“We copied what was done by other countries related to restrictions and regulations,” said Tankiso Motipi, a Civil Registration Officer at the Ministry of Home Affairs in Maseru, Lesotho. “But when it comes to the government going on out to prepare for all the resources, we provided zero resources.”
She said the government of Lesotho was quick to react and follow pandemic procedures, but it failed at the administrative and public health level. Motipi said the first case appeared around October 2020, so the government had time to prepare for cases, unlike other parts of the world.
“There was nothing that we did to prepare for such an event, and all we could do was just cry,” Motipi said.
The government promised to provide masks, hand sanitizer, test kits, and other essential PPE items to reduce the spread of the virus through a government fund and donations, but Motipi said citizens never received any of it.
With little information given to inform the public about the virus, most people were uncertain of everything. The news of the virus didn’t reach the most rural parts of Lesotho until much later in the pandemic.
“At first, it was panic. We were all panicking, we were paranoid. I mean, the whole country because we didn't even know what we were dealing with.”
Motipi said most Lesotho citizens do not have medical aid or insurance. Only people who can afford it have medical insurance.
When it comes to testing for the virus, most people can’t afford to test if they display symptoms because it’s done privately.
Motipi described the only two ways to test publicly, which would be if an elderly person is traveling to receive pension or if someone with severe symptoms of the virus was referred to South Africa for treatment. Those are the only ways to test in a public hospital for free.
“We have only one ICU unit in the country in the biggest hospital which, by the way, is a referral hospital,” Motipi said. “You don't just run to that hospital and say hello, I'm sick. Someone has to refer you and the ICU unit has only nine beds.”
Vaccine diplomacy
The experience in Lesotho contrasts with high accessibility to COVID testing in developed nations, which have testing widely available at most hospitals and pharmacies.
In the beginning of the pandemic, most early COVID-19 deaths and cases were undercounted. Many developed nations have higher case and death counts than developing nations because of their ability to mass test and properly register causes of deaths.
Vaccine diplomacy efforts are determined by sending vaccines to strategically important places around the world. Many countries like China, Russia, India, and the United States have taken these initiatives that are ultimately stunting the ability of underdeveloped nations to stop the spread of the virus.
In some cases, China is selling its vaccines to countries in Southeast Asia instead of donating them.
“We’re sitting on a vaccine waiting for people to change their minds,” Mokdad said. “As many people are dying and waiting in line to get the vaccine. Equity is very important.”
Developed countries have prioritized domestic herd immunity above global health equity, despite the call for international cooperation.
The experience in Lesotho contrasts with high accessibility to COVID testing in developed nations, which have testing widely available at most hospitals and pharmacies.
In the beginning of the pandemic, most early COVID-19 deaths and cases were undercounted. Many developed nations have higher case and death counts than developing nations because of their ability to mass test and properly register causes of deaths.
Vaccine diplomacy efforts are determined by sending vaccines to strategically important places around the world. Many countries like China, Russia, India, and the United States have taken these initiatives that are ultimately stunting the ability of underdeveloped nations to stop the spread of the virus.
In some cases, China is selling its vaccines to countries in Southeast Asia instead of donating them.
“We’re sitting on a vaccine waiting for people to change their minds,” Mokdad said. “As many people are dying and waiting in line to get the vaccine. Equity is very important.”
Developed countries have prioritized domestic herd immunity above global health equity, despite the call for international cooperation.
